Menopause
Written by Marci Mangold, PA-C
Did you know that only half of women aged 50 continue to have intercourse, and by age 70, only 27 percent are sexually active? According to a study at Johns Hopkins, this is a natural effect of aging, and it is not surprising that the older we get the less interest women have in sexual activity and are overall less physically active. Shifting hormones during menopause causes significant changes throughout the body, leading to heart disease, osteoporosis, weight changes, and increased urinary tract infections.
After menopause, approximately half of women experience vaginal dryness leading to increased problems with lubrication and painful intercourse. Although your body may be changing, these effects don’t have to disrupt sexual intimacy with your partner.
We commonly refer to “perimenopause” when discussing these many changes. This is when hormones start to decline, and menstrual cycles become erratic and irregular. “Menopause” doesn’t actually occur until 12 months after your last period, and because you can still get pregnant, continue using contraception until then. According to the American Menopause Society, menopause occurs between ages 40-58, and the average age is 51. Reaching menopause is a process that takes an average of 4 years and can vary from a few months up to 10 years, and after this, women are considered to be in “postmenopause.”
Although this process is different for every woman, most usually experience some symptoms due to the fluctuations and ultimate decline of estrogen and progesterone. According to the National Institute of Health (NIH), about 45% of women experience psychogenic symptoms, which include anger/irritability, anxiety/tension, depression, sleep disturbance, loss of concentration, and loss of self-esteem/confidence. Furthermore, approximately 75% of women experience vasomotor symptoms such as hot flashes, night sweats, palpitations, and migraines. Vasomotor symptoms are considered systemic symptoms (affecting multiple body systems) and usually respond to hormone replacement therapy and will be discussed in more depth in a later 406 Woman article.
The remainder of this article will focus on urogenital symptoms (affecting the urinary and genital regions), which typically respond to localized treatment of the tissues and are experienced by approximately 60% of women.
During menopause, the decline in estrogen frequently leads to thinning of the tissue or atrophy (a literal “wasting away” of tissue), which causes several urogenital symptoms. Urethral atrophy results in urinary stress incontinence (leakage of urine due to the stress of laughing, coughing or sudden movement), urge incontinence (sudden strong urge to urinate results in loss of bladder control before you reach the bathroom), urinary frequency or painful urination.
Vaginal atrophy is another result of this decline in estrogen, which causes less vaginal lubrication and decreased elasticity of vaginal tissue, and in some cases, the vagina may shorten and tighten at the opening. This may lead to symptoms such as vaginal dryness, itching or irritation, tightness, and vaginal pain with burning or soreness during or after intercourse. This often leads to chronic inflammation, irritation, and discomfort, along with tearing and bleeding of the tissue.
Furthermore, these symptoms often lead to avoidance of sex; however, maintaining regular intercourse is helpful to keep tissues strong and lubricated and preserve the length and width of the vaginal space.
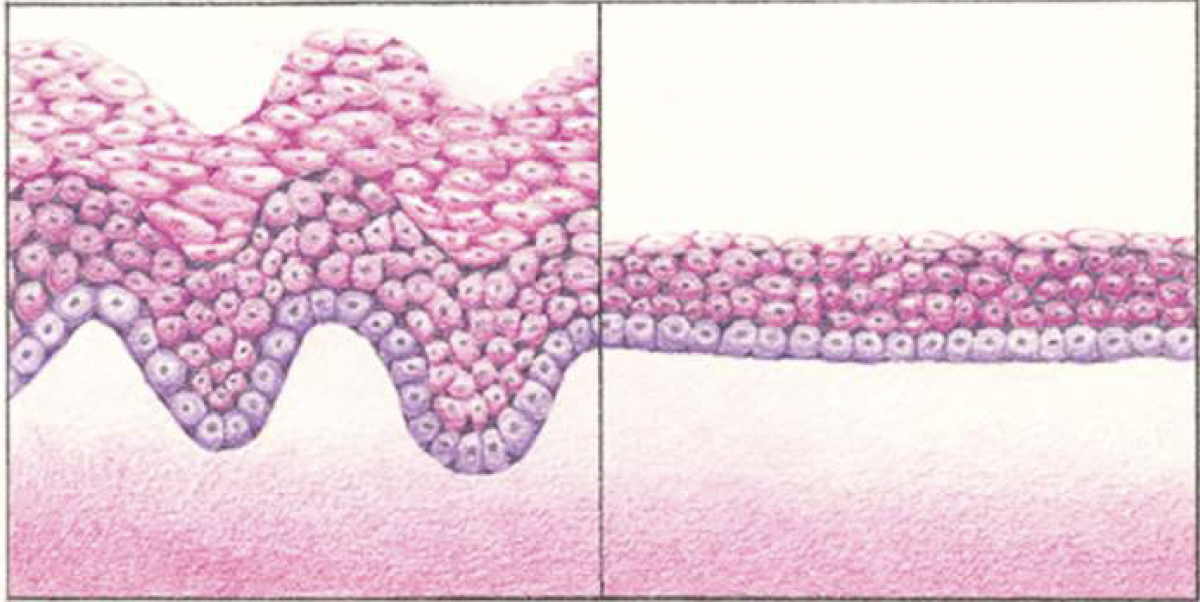
The lining of the vagina before menopause (left) and after menopause (right). Before menopause, when the vagina is well supplied with estrogen, its lining is thicker and has more folds, allowing it to stretch with intercourse and childbirth. After menopause, when levels of estrogen are low, the vaginal lining is thinner and has few folds, which makes it less flexible. (Source: NAMS, North American Menopause Society)
There are several other things you may do to lessen the effects of this low-estrogen state. For starters, always use an excellent vaginal lubricant during sexual activity. Water-based lubricants (Astroglide, K-Y Jelly, Slippery Stuff) or silicone-based lubricants (Pjur, ID Millennium) are recommended since oil-based lubricants (Elegance Women’s Lubricant, Simply Slick) cause breakdown of latex condoms.
Also, vaginal moisturizers can be used 2-3 times per week and will provide lubrication for a longer period of time, typically 2-3 days. Moisturizers often contain hyaluronic acid and are contraindicated only if you have an allergy to the specific product ingredients (examples include Replens, Vagisil, Moisturizer, Feminease, Moist Again, K-Y Liquibeads, HyaloGYN).
If symptoms persist and are significant, then ask your healthcare provider about prescription treatment options. Atrophic vaginitis usually responds well to treatment with topical low-dose vaginal estrogen (rings, creams, tablets or capsules) or dehydroepiandrosterone (DHEA). Vaginal estrogen therapy is the most effective treatment for moderate to severe symptoms. Estrogen therapy restores vaginal pH, thickens tissue, increases secretions and resolves dryness and painful intercourse and reduces the frequency of urinary tract infections along with symptoms of overactive bladder. According to Up-To-Date, long-term data shows no increased risk of breast or endometrial cancer, coronary heart disease, stroke, or blood clots with the use of vaginal estrogen because systemic absorption is low. Despite this fact, vaginal estrogen carries a “box warning” about possible increased risks of these events.
If you have a history of estrogen-dependent tumors or are on antiestrogen therapy, then you should discuss the use of vaginal estrogen with your oncologist first. Although there is more safety data and clinical experience with vaginal estrogen, an effective alternative hormonal medication is vaginal DHEA. DHEA is dosed daily (as opposed to twice-weekly estrogen) and is associated with a slight increase in circulating DHEA, testosterone, and estrogen levels, so it is commonly less preferred and raises some concern in patients with/at risk for estrogen-sensitive malignancies, especially for patients being treated with certain medications for breast cancer. DHEA may be an especially good option for those with low libido. Other treatment options may include daily oral ospemifene (may cause systemic side effects and may increase the risk of breast cancer or blood clots), vaginal testosterone (none are FDA approved for use in females), and laser or radiofrequency devices (the safety and efficacy of these devices remain uncertain). Systemically absorbed estrogen is another treatment option; however, hormone replacement therapy goes beyond the scope of this discussion and will be addressed further in future articles.
In summary, vasomotor, urogenital, and psychogenic changes occur throughout menopause that affect our sexual desires and ability to enjoy intercourse. Decreased estrogen levels lead to vaginal atrophy and is responsible for numerous postmenopausal symptoms. However, a satisfying sex life and relational intimacy can be maintained by adequately treating perimenopausal symptoms. Treatment options include OTC remedies such as vaginal lubricants and moisturizers, as well as prescription treatments with topical low-dose vaginal estrogen or DHEA. Appropriate treatment allows most women to remain sexually active into their 70s and 80s and enjoy the intimacy that a mature relationship provides.
If you want to discuss your health through menopause, we’re here for you!
Call our office at 406-752-5252 to schedule an appointment.
*This article is orginally published at 406 Woman magazine Nov/Dec issue